 Why are FAMILIES and mental health advocates of loved ones WITH SERIOUS BRAIN DISORDERS fighting so hard FOR RECLASSIFICATION?Recently, the term Serious Brain Disorder (SBD) has been circulating in my Facebook mental health advocacy groups more and more. At first, it seemed as if these circles of advocates wanted the insurance companies to code Serious Mental Illnesses (SMIs) differently so they would issue better compensation to psychiatric providers and so patients could have easier access to treatment. In that case, I thought, why not address it with how the insurance companies are required to code them? But it starts elsewhere, beyond the insurance companies. As I explored and researched the issue, it became clear that taking Serious Mental Illnesses seriously must include labeling it transparently and as unbiased as possible. Here are several reasons why families and mental health advocates of loved ones with Serious Mental Illness—especially schizophrenia and the like—are fighting with all their hearts, souls, and minds to have it recognized as what it truly is: Serious Brain Disorder. First, What is SMI?The Diagnostic and Statistical Manual of Mental Illnesses defines Serious Mental Illness as “a small subset of the 300 mental illnesses that are in DSM.” “According to the National Institute of Mental Health, serious mental illness is relatively rare, affecting only 5% of the population over 18. Serious mental illness includes schizophrenia; the subset of major depression called ‘severe, major depression’; the subset of bipolar disorder classified as ‘severe’ and a few other disorders.”(4) One of the sources I interviewed pointed out that the general public doesn’t know what Serious Mental Illness is so reclassification would clarify the concept. On the other hand, I pointed out, wouldn’t that muddy the water? Not if they are educated. SBD EffortsAn organization advocating for the reclassification of SMI to SBD is the National Shattering Silence Coalition (NSSC). The nonprofit has eight points of unity members align under, and the first is their primary concern:
The Two Were Once OneThe two disciplines—neurology and psychiatry—are not as different as one may think. In fact, at one point they were one discipline. Historically, psychiatry and psychology were a part of neuropsychiatry until “psychiatrists enthusiastically embraced the key that they were given to the human psyche, and this new ‘mentalistic’ approach consequently detached psychiatry from neurology,” this article in neuro.psychiatryonline.org explains. “It may be further speculated that neurologists, too, accepted this dichotomy and were relieved to leave the treatment of mental illness to others.”(1) A Broken System Slighted and MisunderstoodMental health and the demand for psychotherapy and psychiatry are coming into the forefront on matters related to COVID-19’s mental toll on peoples’ psyches. However, advocates for SBD have been begging for practical solutions to a broken mental healthcare system long before the present worldwide crisis. Jeanne Allen Gore, SBD advocate, co-founder, and Coordinator of NSSC, argues that mental healthcare as an industry has been misconstrued, underfunded, and at a large disadvantage from neurology and pathology sciences and healthcare systems. Gore points out, “If you do the math, there is a glaring mismatch: $36.55 spent on adults with SBD compared to $478 on those with Alzheimer’s, which is 13 times, or 1,327% more per person.” According to Gore, other brain disorders like Alzheimer’s and autism have been inclined to more empathetic responses from the public. Since Alzheimer’s and autism have been funded and fought for their position at the table of medical sciences to be recognized as structural, biological, and medical brain disorders, it appears they garner more compassionate attitudes and legitimized views from society. The Science Has Been ThereIn the article at neuro.psychiatryonline.org, authors Shahar Arzy, M.D., Ph.D., and Shlomo Danziger, M.A. explain, “With our current scientific understanding of the cerebral basis of psychiatric disorders, the era of the computational, data, and genomic revolutions once again merges the domains of neurology and psychiatry for a neuroscientific-based diagnosis, monitoring, and treatment of neuropsychiatric diseases.”(1) In regards to SBDs like schizophrenia and symptoms like psychosis, science and technology are making ways to merge the disciplines of neurology and psychiatry. Especially in disorders like schizophrenia, severe depression, and severe bipolar disorder where psychosis is a symptom, these are brain-based and medical in nature. “More recent and dramatic evidence has come largely through functional magnetic resonance imaging and positron emission tomography,” per Mary G Baker, President, European Parkinson’s Disease Association as stated in Baker, Kale, and Menken.(2) Mary Palafox, RN, Chair of the Schizophrenia and Psychosis Action Alliance (S&PAA) states, “It’s not a debate whether schizophrenia is a neurological illness. Science has already determined schizophrenia to be a neuro-developmental disorder.” You can visit their website over the next few months and follow how S&PAA is actively changing the treatment paradigm for those with schizophrenia spectrum disorders. A Legal Loophole and Political ProblemsYet in practical solutions to psychosis in schizophrenia, psychiatrists cannot treat psychosis if the patient is not voluntarily admitted or concedes to treatment by their own will. In any other discipline, in a state of psychosis as a result of a medical condition, the doctors must treat, and their hands aren’t tied by laws. The danger of the legalities with SMIs or SBDs is what happens to many with SBD like schizophrenia when untreated, known as “dying with their rights on.” Jeanne Allen Gore writes: “People with neurological illnesses, under medical standards of care, have access to resources and supportive care that those diagnosed with a ‘mental illness’ do not have access to. Their doctor makes the decisions about what level of care is needed and when it’s needed, not a judge. For decades, the decision to admit a patient with SBD for medical care has been made based on laws requiring dangerousness and the availability of hospital beds, or should I say, lack thereof, rather than medical necessity.” She emphasizes, “This unconscionably cruel system has resulted in horrific abuses, neglect, and suffering. Our loved ones end up homeless, incarcerated, or dead far too soon. Science has proven these are no-fault, neurological brain disorders. Clinicians, doctors, and scientists know this. They are not a failure to control one’s behavior, a character weakness, or the result of a traumatic childhood.” Behavioral and mental health sciences have their value in psychosocial rehabilitation for substance use. Psychotherapy continues to be a respected and evidence-based approach for those with cognitive damage and disorders from substance use, trauma, and brain injury. The value of psychology and psychiatry cannot be ignored and compartmentalized, and there is a place for all these studies to effectively work together to help patients and those who care for them. It won’t be achieved as effectively and as successfully if true severe, serious mental illness, is not taken seriously in and of itself. To do that, action must be taken to move psychiatry and neurology back into a working relationship. The advances in science are here and there is enough evidence to show the validity of a medical cause of schizophrenia and these types of severe illnesses. The Bottom LineThe battle to have SMI recognized as SBDs continues, in order to be funded for more research to find better treatments and more physical tests connecting the symptomology of psychosis to the etiology (causes) of biological and physical structures. When the standard world health organizations take serious brain disorders seriously, then doors can open to more changes and better care. Then insurance payers can code them “medical” and doctors in hospitals and ERs will have to treat them as any other medical condition: with integrity, compassion, and ethics. Advocates for SBDs are pleading for this shift in terminology and semantics because of the severity of the illnesses and the brokenness of the system that currently treats those with them. With language that articulates that these disorders are brain-based and physical, reclassifying SMI to be recognized through medical standards can lead to better care and more practical solutions for individuals who suffer from it. This will level the playing field for equity in research and treatment funding, awareness campaigns, and give access to care and programs like #HousingThatHeals, just as Alzheimer’s and autism have achieved. With every discovery we make to understand mental illness, we will all inevitably have to face the reality that “mental” is medical. Reclassifying Serious Mental Illnesses as Serious Brain Disorders is the gateway to the broader acceptance of that reality. references
addendum from Kerry Martin, CEo & FounderAn added benefit of reclassification is removing the word "mental" from our narrative which would erode stigma in our society — in our workplaces, schools, social media, etc — saving lives and lessening suffering for our children, youth and adults struggling with their mental health. Stigma is trapping far too many behind its wall in silence and in shame, keeping those in need from reaching out for help. And, for those who believe we have made great strides in eradicating stigma, I would ask you, why hasn't our own Congress repealed a blatantly discriminatory law that has been on the books for almost 60 years, the IMD Exclusion, that has resulted in marginalizing our most vulnerable citizens, incarcerating them in our jails and prisons, walking over them on our cold streets, and pushing them into early graves?
0 Comments
2/7/2022 A Personal Message to All Struggling, Especially teens and Young Adults: I See You, I Hear You, AND If My Words Could Make a Difference, This is What I Would Say to YouRead Now If you were having symptoms of a heart attack would you call yourself “crazy” or would you call 911 and get help? Here’s what I would do. I would definitely not be calling myself “crazy.” I would be calling 911, telling them it was an emergency, that my life was in danger, and I need an ambulance and paramedics sent as soon as possible to get me to the hospital. If I could not call, my loved ones or friends would call. Even a stranger would call if they saw me collapse. If I saw someone in such a crisis, I would make the call to 911 myself. And what if medicine or life enhancing therapies such as nutrition, exercise, sleep, and stress reduction could help save my life? I would ask my doctor to educate me on the best “heart health” practices. I’d ask for prescriptions and referrals because I want to stay alive, be healthy, and I don’t want to die. So why do we insist on thinking our brain is not part of our body and act so differently when our brain health is at risk? Why do we dismiss or hate ourselves and/or think others will ridicule and/or shame us if we have a “mental” illness? Maybe in part it’s the stigma we feel and fear we’ll feel that’s so associated with the words “mental” illness. I don’t like how that word has been used. It’s said in disparaging ways, in unkind, and untrue ways - as in - she’s “mental” and he’s “mental.” “Mental” meaning “crazy” - less than human - an aberration. Being “other” than everyone else. “Just pull yourself together. Snap out of it! Stop wallowing. I’ll give you something to really cry about.” That’s some of the unhelpful comments we hear. And how about, “It’s all in your head?” Meant as a put down, but in reality, yes, that’s true. Inside our head is our brain and it needs help not sarcastic, shaming, or demeaning remarks and criticisms. Do I call my lungs “crazy” when I’m having an asthma attack? Definitely not. My lungs are not well, yes. But crazy? No. And what do I do to help myself? I’ll use my inhaler. If I’m still in an acute crisis - as in - I’m wheezing so much that I'm having real trouble breathing, I’ll get myself to an emergency room. Will I be ashamed of being asthmatic? No way. I will tell the nurses and doctors I have asthma and ask for medical help. How different, though, it can be for psychiatric illness that strikes at the brain. It’s essential to remember that the brain is part of the body. “Mental” illnesses are in reality physical illnesses. Our brain and our mind may suffer, but that does not mean we are “looney tunes, crazy, or nuts.” After all, the brain impacts our whole being - how we think, feel, act, speak, eat, sleep, and more. Think of it this way. When our brain is attacked from inside itself, we might experience a depression attack, manic attack, anxiety attack, panic attack, suicidal attack, self-hatred attack, what’s the point of living attack, an urge to self-harm attack, body image distortion attack, and other such “attacks” whose source is invisible from the outside while all too painful and real from the inside. Our brains are not “crazy.” These types of attacks are just as real, just as important, and are just as in need of help as when we have a heart attack. A heart attack can be life threatening. A brain attack can also be life threatening in terms of life and death, as well as the on-going quality of how we are able to live our lives. Let me ask you this. Do you know that suicide is the 10th leading cause of death in the United States? Here in Oregon where I live, the number one cause of death for ages 10 to 24 years old is suicide. These deaths did not have to be. The flesh and blood lives that could have still been lived now forever lost into the abyss of suicide. We must be vigilant and aware of “psychiatric brain attack” warning signs such as change in mood, suicidal thoughts and actions, self-harming, change in sleep and eating, alcohol and drug use, anxiety, panic, and despair. Our brain deserves respect, and it deserves help. We deserve our and others’ understanding and compassion, and not the cruelty of being shamed. Silence, shame, and stigma need to be banished. That will happen when the truth about psychiatric illness is known and we bravely share our mental health stories. Let’s make everyone aware that illness attacks on brain health are real. They can be life threatening and should be approached just as one would any other health crisis. Now that you know the truth and that medication and/or therapy help is available, please don’t become a statistic. Save your life. That’s what your brain and your heart want you to do. Have my words made a difference? I pray that they do. Your voice has power in The “If My Words Could Make A Difference” Youth Mental Health Campaign.
Teens and young adults can share their own creative pieces of work or view those submitted by others on ASHA International's website. They can not only be part of the conversation but help lift their peers up as well. Our youth are in a crisis, with a national emergency declared. please share OUR message and THIS campaign.Please share our message as well as this youth campaign with those who may benefit from hearing it or taking part in the conversation, and sharing their story. Let's all be there during this National Emergency for Youth Mental Health. Our youth are in a crisis. We cannot let them down. Let's remind them: "You are important. Your thoughts, feelings, and observations are important. You can make a difference. What if your ideas could help change the world? What if your ideas could help improve the life of just one person? Would it be worth it? We think so!" Do you need help now? Please reach out. help is available. Poster by Diane Kaufman and Amanda Meador. If you're in a crisis, please reach out now. Call the National Suicide Prevention Lifeline 24/7 at 1-800-273-8255. Or, to connect with a Crisis Counselor, text HOME to 741-741. You can do this. You matter. AuthorDr. Diane Kaufman, MD, Child Psychiatrist, Humanism in Medicine Awardee, Founder-Director, Arts and Healing Resiliency Center, Mind Matters, PC; and, Suicide Prevention Collaborator, Accelerating Social Good. 2/2/2022 PRAYER WORKS BUT SO DOES COUNSELING: Let’s Normalize Seeking Help for our mental health in THE Black Community SO ANOTHER GENERATION DOESN'T suffer in silenceRead Now Photo by RODNAE Productions from Pexels OUR GRANDPARENTS MADE US FEEL ASHAMED WE NEEDED HELP BUT HOLY OIL CANNOT FIX EVERYTHINGLet’s talk about this. In all honesty, there are several reasons why there is such a huge stigma associated with mental health, especially in the Black community. Mental health probably was never a topic of conversation for many black families. If the topic did come up, our grandparents would just throw some holy oil on us and pray. They felt that anything out of the normal was demonic. The foundation of mental health among many black people can be traced back to times of slavery. In reading about history, I can't help but imagine many slaves suffered from severe anxiety, depression, as well as other mental illnesses. We need to stop telling each other WE'RE OKAY WHEN WE'RE HURTING INSIDEThis issue of masking mental illness is prevalent in the black community. The majority of us who suffer from mental health struggles in the black community suffer in silence due to stigma. Speaking from experience, I grew up in a culture that tells us “we are to be strong,” that we “should deal with problems on our own.” This only enforces the idea that it is not okay for us to say we are hurting inside. I have spoken to countless friends who say “you don’t suffer from mental health illnesses and you should pray.” I do pray, daily. However, I also need to be realistic and understand that I do suffer from mental illnesses. I do need to seek additional help, such as counseling.
Why aren't African Americans seeking mental healthcare?Approximately, 25% of African American seek mental health care compared to 40% of whites. Why is this? According to Mental Health America:
BLACK CELEBRITIES SPEAKING Out ABOUT THEIR MENTAL HEALTHLuckily, in recent years, more and more black people, including those in the public eye, have opened up about dealing with and overcoming the struggles of mental illnesses. During an interview with Essence Magazine in 2018, Janet Jackson, noted that depression and feelings of inadequacy have followed her since childhood. In 2013, former Destiny's Child member, Michelle Williams, revealed she has been battling depression since she was a teenager. She has since become a mental health advocate and has spoken about her struggles openly on many platforms. it's okay if you're going through something. it's even better if you seek help.I believe God-gifted people -- physicians, doctors and therapists -- to assist in our healing. Please go see a professional so that they can assess you. It's okay if you're going through something. It is even better to seek help. You don't need to tough it out. It's not cute to walk around knowing you need help but won't seek it because of what others may think. Other people's opinions of you are their issue, not yours. by not opening up about our mental health, we're saying it's okay for ANOTHER generation to GROW UP WITHOUT help.If we are unable to remove the negative stigma surrounding mental health in the black community, we are willingly allowing another generation to grow up without access to counseling and mental health resources that can help them live a happier and healthier life. In order to end the stigma of mental health, we need to have candid conversations surrounding mental illness. I do not think many of us are aware that mental health is a physical disease and it affects us in more ways than we think. People need to be educated. I have had conversations with friends who do not understand why I suffer from mental illness. I'm the one who has to educate them as it's extremely important to do so. The black community should not be afraid to have these types of discussions. These conversations should start in the household and be held without judgement. Let’s start having conversations first and then we can move on from there. resources for our communityreaching our national hotlineNational Suicide Prevention Lifeline: 1-800-273-8255 Crisis Text Line: Text HOME to 741-741 to reach a Crisis Counselor AuthorDr. Meagan T. Copelin is an international speaker, author, empowerment coach, blogger, contributing writer and podcaster; and we are honored to have her serve as our Supporting US Chair for Accelerating Mental Wellness, our social change campaign to co-create stigma free workplaces built on a foundation of empathy with needed mental health supports and programs. Meagan is also the Founder of Mental Rich, a mental health company and brand, dedicated to helping young girls and women who suffer from mental illnesses steaming from abuse, abandonment, and rejection. Her calling is to become a trailblazing voice for young girls and women worldwide. Drawing on her own experiences of mental illness due to abuse, rejection, and abandonment, Meagan uses her words to encourage others to build a home within themselves; and, to love, live, and create fearlessly. Her advocacy projects and efforts have helped her to be featured on several platforms for the purpose of empowering women to tell their story from struggle to success and live up to their full potential. 1/31/2022 So Many Hearts Ache for Lives Lost to Suicide THAT We, The Living, Must Shine a Healing Light on Silence, Shame and Stigma: AN Interview with Child Psychiatrist, Artist and Poet, DR. DianE Kaufman, MDRead Now Hope lives. shame kills. everyday is suicide prevention day for Dr. diane kaufman, MD.Kerry: As suicide survivors and mental health advocates, Lucia and I both so deeply appreciate your tremendous body of work in suicide prevention. Your award-winning poems, songs, posters, videos and even an opera have inspired hope, encouraged people who are hurting to reach out and offered solace to those who have lost a loved one to suicide. Can you tell us why suicide prevention plays such a prominent role in your life and work? Diane: In August 2019, my friend and mental health colleague Stacy ended her life by suicide. Her tragic death was and still is a shock to me. Stacy was a psychiatric nurse practitioner of great skill and compassion. I respected and admired Stacy for having so many positive qualities. I used to tell myself, if a family member of mine needed care, I would send them to Stacy. Her taking her own life and leaving behind two sets of young twins was absolutely one hundred percent out of character for Stacy – the woman, friend, and mental health professional - that I knew her to be. What ended Stacy’s life – what devoured, destroyed, and killed her – was depression. Even as I say these words, tears come to my eyes. I still can’t believe she is gone. Depression is a physical illness that invades the mind, body, and spirit. And, it can kill.
There, however, have been other significant events. When I was a medical student, I attempted suicide, and was medically hospitalized. When I was married, my father-in-law killed himself by gun shot. My teenage patient, who seemed to her mother, her teachers, and to myself to be doing so well, hanged herself in 2016. The best friend of my young adult patient died by overdose in 2020. My patient, who had her own history of suicide attempts (prior to when I began treating her), found her friend, and then became at increased risk for suicide herself. All of these tragic events have transformed me into a suicide prevention activist. poetry transforms depression and despair into Healing and hopeLucia: Why do you choose to express yourself through poetry? And, what was the impetus behind writing the poem, “Don’t Give Up” which you would later turn into lyrics with a song-writer and then two Suicide Prevention Public Service Announcements (PSAs), both a one minute version and a longer five minute version, in hopes that people would share the PSAs far and wide to help those who were struggling?
Diane: I turn to poetry to express myself when I am feeling overwhelmed by thoughts and feelings. It’s a way to safely get what is inside of me – what’s troubling me – out into the world and onto a page. It often feels like the poem is a living thing wanting to communicate and be expressed, and I am the one listening and holding the pen to let it out – to be taken in and experienced by another. “Don’t Give Up” was an outpouring of my heart listening to the sadness, depression, despair, and suicidality of my youth patients. It’s a conversation with a suicidal person. The poem is saying even though you want to kill yourself, please don’t do it because I understand how you feel, and I know that your choosing death is not the answer. There are reasons for you to keep living and people who truly care and can help you. 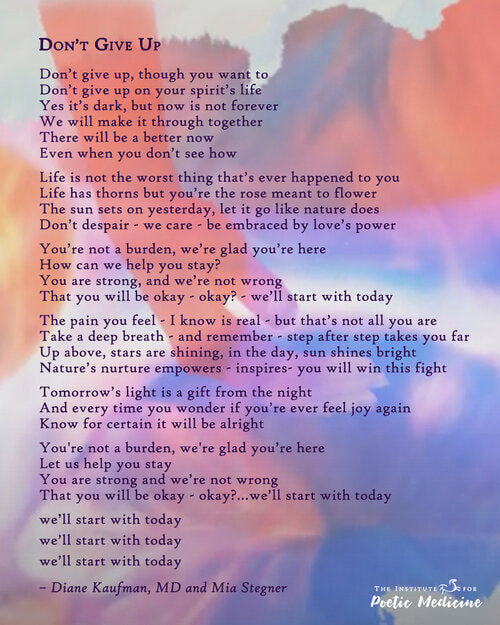 How do we convince those feeling hopeless to not give up?Kerry: There is a quote by Hal Lindsey, “Man can live about 40 days without food, about 3 days without water, about 8 minutes without air, but only for 1 second without hope.” Not surprisingly, hopelessness is the leading predictor of suicide. Speaking as an attempt survivor, I can certainly attest to that being the case for me. For months on end, I battled with feeling like there was no hope that anything was going to get better, no hope I was going to feel anything other than this unbearable sense of loneliness, bleakness and foreboding, no hope for a better tomorrow … really that there was no hope for me. And, then to see those I love seeing me that way and not knowing how to help me was just too much to bear. I was not only hurting but I was hurting them. How do we get people to not give up and give into these feelings of hopelessness? Diane: The first line of the poem/lyric is “Don’t give up even though you want to.” Many people – maybe all people – have at times felt like giving up - wishing they were never born, wishing they could just sleep forever, wishing they could be dead, and for some – wanting to end their emotional pain by killing themselves. I want the person listening to the song to feel the song is being sung just for them. For them to know they are not alone in feeling hopeless, and yet also to know that this day is not forever, there will be another day and life can change for the better. As long as there is life and there is help available there is hope. Suicide is forever. The severe emotional pain coming from depression and/or severe life stressors can be helped, lessened, and improved while we are still alive. We don’t have to kill ourselves to stop the pain. I know this to be true as I have lived it. When we are depressed, our thinking gets distorted and it’s as if all we see is darkness. It’s important to be compassionately reminded that, “There will be a better now even when we don’t see how” and that “Tomorrow’s light is a gift from the night.” What more can we all be doing to help our CHILDREN struggling with their mental health?Kerry: Given your specialty is child psychiatry and you see in your practice teens who struggle with suicidal ideation or who have attempted to take their own lives, what more do you think we need to be doing to help our kids given suicide rates are increasing in this demographic? In October 2021, the American Academy of Pediatrics, American Academy of Child and Adolescent Psychiatry and the Children’s Hospital Association declared a national emergency in youth mental health. This declaration should inspire and galvanize us to collaborate on behalf of youth mental health by improving access, services, and resources. We need more mental health providers and services available. We need more in-patient psychiatric beds available, as well as a higher level of care and specialty programs. Social media can damage youth mental health when self-worth is judged by “likes” and when sense of self and self-esteem plummets by negatively comparing ourselves to online profiles of others. Youth need healthy social connections and to experience themselves as worthwhile. They need caring adults who will ask the questions – “Are you okay? Are you feeling anxious and/or depressed? Are you thinking about hurting, cutting, and/or killing yourself? You can tell me because I care about you.” Youth need to know there is no shame in seeking help and that mental health is physical health and help is available. Mental health education should be integrated into all school settings. There are skills and coping strategies we all need to learn and practice. We also need to understand the warning signs of mental illness so we can better recognize when things are not okay with us. honoring and practicing THE human art of connection To promote mental health and NUTURE resiliencELucia: Diane, you have also worked for many years as a Child Psychiatrist back East and now in Oregon, and have extensive training in the therapeutic use of poetry, art, and story. Now, as Founder and Director of the Arts and Healing Resiliency Center at Mind Matters, PC, how are you working to eliminate silence, shame, and stigma to prevent suicide? Mental health well-being can be nurtured in many different ways. I have Bipolar II Disorder, attempted suicide as a young adult, and became a child psychiatrist. Sharing my story helps break through silence, shame, and stigma. I am an ASHA International storyteller and am on their Board of Directors. It’s a great organization that highlights the “superpower” of our personal mental health stories. The expressive arts can also play a vital role in facilitating and fostering mental health. The inspired mission of the Arts and Healing Resiliency Center is to honor and practice the caring art of human connection. The ARTS Program, our unifying concept, inspires Adolescent and Adult Resiliency Training as well as Skills and Support by interweaving evidence-based mental health skills, positive psychology principles, and the creative arts to promote, nurture, and build mental health and life affirming resilience. The goal of the program is a felt sense of personal integrity, authenticity, and responsibility leading to social-emotional and behavioral well-being. We offer online workshops, special events, mentoring, and therapy.
AuthorSKerry Martin, CEO and Founder, and Lucia Martinez Rojas, Social Media Strategist and Videographer, Accelerating Social Good with guest Diane Kaufman, MD, Child Psychiatrist, Humanism in Medicine Awardee, and Founder and Director, Arts and Healing Resiliency Center, Mind Matters PC. 12/15/2021 EMPATHY AND KINDNESS IN our WORKPLACEs priceless: WHAT WORKING WITH STIGMA FREE LEADERSHIP LOOKS LIKE when you have undiagnosed major depression, anxiety, add and an eating disorderRead Now We have an advocacy campaign running to eliminate stigma in the workplace and create cultures based on kindness and empathy, and have published a number of blog posts speaking directly to our team's lived experience with workplace stigma and the negative impact it has on their lives (such as being fired after CEO finds out our India Chair has bipolar disorder and a suicide attempt after our US Chair is laid off whilst in throes of major depressive episode.) This is a different story however - one based on working in a stigma-free environment with my lived experience, mental (read physical) illness and an eating disorder. What I was up against: undiagnosed inattentive ADD, social anxiety, major depression, and an eating disorderI was working for a large building corporation that had umbrella companies such as telecommunications and facilities management. While I had a direct manager, I also had the Chief Operations Officer who managed me (and the entire company). At the time I was living with undiagnosed inattentive ADD, generalised and social anxiety and major depression. I was also living with an eating disorder for which I needed intense treatment. While I was seeing a psychiatrist during this time, he diagnosed me with depression. That was all. Little did I know the depression was slightly more than just your everyday depression. Major depression sucks but it would take another five years before I was formally diagnosed with this. My bosses put my wellbeing first when I seek treatment for my eating disorder even thou pain in the ass for my co-workers.After working in the Business Centre of this company I got a promotion and moved into the Telecommunications office. It was an all male office except for me. I was the only female. At first I was my normal self - quiet because I was anxious and trying to find my feet in this different part of the company. Once I felt comfortable and opened up, the boys I worked with became more like brothers than coworkers. We had a lot of fun and laughter. It was during this time that I needed to seek treatment for an eating disorder. This involved missing every Friday morning and having a two-hour lunch break once a week so I could go to a shopping centre and have lunch there with my therapist as my biggest phobia was eating in front of people. This is where the stigma free workplace and management comes into things. Not only did my boss in the telecommunications department support me during this time, but the Chief Operations Officer did too as he had to approve it all. I know it was a pain in the ass for my coworkers but I needed to do this for myself. You have no idea how grateful I was to have the manager I had in telecommunications and the Chief Operations Officer be so supportive of what I had to do. when you google "cats in tights" due to your inattentive add and anxiety, thing start to fall apart. Yet, I was Supported by management once again.I was working with undiagnosed mental illnesses at the time but what really impacted me on a daily basis was my inattentive ADD and anxiety. In a meeting with my COO, he said my performance was like a rollercoaster, that went up then went down again, then up then down. I couldn’t focus on the task at hand and know I would have been the employee they knew I could be if I had been diagnosed and medicated for ADD. My COO took hits for me as well - my performance came into question with the Directors and upper management. I know that he guarded me and shielded me from being fired or disciplined for my work performance. I tried so hard during my time in the telecommunications department, but when you can’t focus and end up googling cats in tights due to your inattentiveness, things start to fall apart. I was moved to the facilities management division probably in the hope my work performance would improve. after making alcohol my best friend, I let that friendship end and elected to resign. But through all this, they never gave up on me.My work did not improve. I was so anxious all the time. Almost every day my friend and I went to the pub at lunchtime so I could have a beer to calm myself down. Alcohol became my best friend during this time because it masked all my emotions and I didn’t need to think about my underlying anxieties. While most people would be fired for this, the company knew something wasn’t right with me. Every Christmas party I would get hideously drunk and black out, not being able to remember the night before. We had an amazing team of people at this building corporation and when I drank I embarrassed every single person I worked with. Sure, I laugh about certain things now, but the reason for my drinking was to hide my mental and emotional pain. I ended up handing in my resignation from the company after five and a half years to pursue real estate, as my family were moving back to Perth and I wanted to stay living in Melbourne. Creating a stigma-free workplace isn't rocket science. If i didn't get the support I did from leadership, I don't know where I would be today.Creating a stigma free workplace isn’t rocket science or hard. This company did it for me so willingly and never ever questioned what I needed to do. They were there to support me and they went above and beyond to do this. There were no questions asked. It was just what I told them I needed to do and they were amazingly understanding. I think on the day I resigned everyone breathed a sigh of relief. I couldn’t continue working there the way I was. They perhaps knew it before I did. But I realized I needed to pause and seek more intensive treatment. I still have relationships with a lot of people from the company today, 15 years later, including my boss in telecommunications and the COO. They now all know about my mental illnesses as I have been very vocal about it, and they are just as they were at work - totally understanding and supportive. They are just all around great people. To rid your workplace of stigma, you just need acceptance. That is all anyone wants. If the shy, anxiety riddled kid starts working below their capacity, ask them if they are okay. If the severely depressed person takes more days off than allowed, ask them how you can help. When people go to management and advise them of their mental illnesses ask how you can make it so that it won’t impact their job. Keep things on a level playing field. I will forever be grateful to my company I worked for and the way they handled me, my mental illnesses (albeit undiagnosed), and my work ethic and behaviour. They could so easily have wiped the slate clean, said this is too much and have somebody else replace me. But they didn’t. They kept their belief in me. I don’t know how or why, but they did. But what I do know beyond a shadow of a doubt is, if they didn’t help me through those hard times with my eating disorder, I don’t know where I would be today. Empathy and kindness go a long way. And, they both cost nothing. My bosses and colleagues giving me the feeling that I was worthy and that I belonged despite my issues was invaluable to me and my mental wellbeing. Really, when you give it a think, aren't we all worthy? Worthy of empathy and kindness? AuthorErin Macauley, Chief Hope Officer, Accelerating Social Good, and Australia Chair, We Are All Worthy, a cause-advocacy campaign to co-create stigma free workplaces on foundation of empathy with needed mental health programs and supports for all. 12/15/2021 Challenges Those with Bipolar Diagnosis Confront in Workplaces: Don't Let Anyone Tell You This Is Not the Right Job for YouRead Now perhaps this isn't the right job for youI have been told that, “perhaps this isn't the right job for you.” Don't let anyone tell you that. And if they do, do not believe them.
I work well. I am a good employee. Let me give you a small list of jobs that I have done that I have had panic attacks during: waitress, delivery driver, warehouse, janitor, social worker, zookeeper, ride operator, cleaner, canvassing, lab tech, cafeteria worker, retail, student, and mother. That is a wide variety of jobs. If I believed that I could not work somewhere because I was going to have a panic attack, then I would not be working. I work anyway. just because my panic attacks my make some uncomfortable is no reason for me to hide in my house and not work.I have bipolar disorder and it affects all parts of my life. That is something that I am constantly trying to manage. Just because that may make someone else uncomfortable, it is not a reason for me to hide in my house all the time. Some people cannot work and there is no shame in that. I cannot go to any other grocery store than my one grocery store. There is no shame in that. We all have our difficulties and if yours is that you cannot work, I respect that. But, perhaps, maybe you can go food shopping, but you occasionally have a hard time. Should you have to order your food and have it delivered? Of course not. if i had a visible illness, would you tell me not to work? of course not.If I was blind would you tell me I cannot work? Of course not. Why is it okay to tell someone with a mental illness that they cannot do something? I have difficulties, it is true, and sometimes I need a little help. I am not asking for special treatment. I am simply asking to play on the same level field. addendum: why we're launched a global grassroots campaign to create stigma-free workplaces built on a foundation of empathy - by the people for the people - to ensure we all feel worthyRaine not only deserves the same level field, she like anyone else with a serious brain disorder or, anyone else who is in need of mental health support (clinical diagnosis or not), deserves empathy, grace, caring and kindness at the workplace. In too many workplaces however, the field is far from level. We also all deserve to work in stigma-free environments that enable us to flourish and do our best work for our employers and for ourselves so we may feel of the utmost value. So we feel we belong. So we feel worthy. Not a total lack of empathy and caring friends. Because we as human beings always deserve that. Always. Today, our workplaces, more often than not, are not safe places. They are not empathetic, kind or caring. And they are chock-a-block full of stigma. Case in point, the Great Resignation where droves are leaving as they don't feel they are getting the deserved mental health support. Whilst it's easy to build a business case for why companies should bring in proper mental health programs and supports, still far too many have failed to do so. But here, we are presenting the human case (or cost). In light of far too many human cases brought forth by not only mental health advocates but ordinary people trying to survive, we have launched an Accelerating Mental Wellness Campaign asking workplaces to take a pledge to meet our criteria for stigma free environments. We are paying attention and watching on behalf of simply too many who are being treated with a total lack of empathy, grace, caring and kindness. And, on behalf of some who have attempted to take their own lives as a result; and on perhaps behalf of some who have died by suicide. We simply will never know how many as their precious souls are no longer here. For more on our global initiative to put an end to workplaces discriminating against those who are simply suffering and in need of empathy not a lack of support or, in the worst case, who are fired for bravely coming forth with their struggles or for not performing due to depression, please see our Advocacy page. And join us our movement to ensure all people feel worthy regardless of need for mental health support by signing our change.org petition: change.org/weareallworthy. We do hope friends that you will join us, stand up and speak out. This simply has to stop. authorAs part of our social change campaign to co-create stigma-free workplaces built on a foundation of empathy with needed mental health programs and supports, we invite people to share their stories with us to help build the human case. We believe we can humanize stigma with storytelling and educate by sharing what is it feels like to walk through our world with a serious brain disorder.  NOTE TO READER. This is a story submission to our Accelerating Mental Wellness Campaign from a stigma fighter. As part of our social change campaign to co-create stigma free workplaces built on a foundation of empathy with needed mental health programs and supports, we invite people to share their stories with us to help build the human case. Please join us in thanking Mehar, who finds within herself the courage to not only share here, but also uploads a selfie to our Wall of Solidarity, taking another brick out of the wall of stigma, signs our We Are All Worthy change.org petition, and shares her reasons why on LinkedIn, asking others to sign too. Mehar, you truly are a stigma-fighter superhero! And, we so love and appreciate you. May your inner light continue to shine on brightly. When manic, it is about wanting to change the entire world and believing I can. I truly live the words “the ones who are crazy enough to think that they can change the world, are the ones who do.” And it is not always a delusion. If I can brace it, channel it and welcome it. I can be just crazy enough. Just a little less crazy than the bad while braver than those who let logic come in the way and play it safe. They say it's in my head and I say yes, you are right, It is! but they don't believe it's true.Would it be truer if your brain was on the outside, I ask? Wouldn’t YOU do everything to protect it …anything that is needed? Why is it on me to teach you when you are the ignorant one? Doctors say “Let’s treat the highs first.” I don’t trust them. I feel exceptionally creative, powerful both physically & mentally. And, oddly spiritual. That to me is the best part. I can read the signs of the universe. But this phase transitions into a paranoia where I think my doctors are conspiring against me, and the entire world is my enemy. It is a constant battle because the highs bring out the best in me but the lows are my enemy. I know they are both liars, and still they are not. Unhealthy high horse of self-righteousness, over-confidence, grandiosity and detachment from reality. The racing, obsessive yet beautiful ideas but that incoherent pressured speech… where they get lost and so does everyone around me. Those profound conversations, my creative hunger! Am I making the best speech? Things I never said before, things I have never ever heard. “So profound” my friends would say, but my poor luck “what, what did I just say?!” lost in a memory fog, I am stuck in the middle of the best version of myself and the worst one.The bickering breaks me down. In my darkest moments, I fear the most, I see my universe collapse, and the signs fade ... no matter how much I stretch my arms. And then the whole sky comes down falling on me. And, for some strange reason, that sky is grey and dark and awfully quiet around me. The tunnel vision, it is surreal. And then, it grasps me in its arms, but it doesn’t want me to know what ‘it’ is. The anxiety feels like a gremlin sitting on my shoulder, whispering lies in my ears every moment of the day. But then the gremlin leaves. I just feel awfully lonely. The memory of my high-self is what keeps me going. I believe in all my dreams, hopes, and thoughts that were racing in my mind, and I pray I will remember them. I know now, from the help of my same therapists, doctors, and the loving community, that this is no illness. This is as humanly as possible I can respond to the miracles and trials of life. there is help. there is hope. But wouldn't it be amazing to seize that just crazy enough moment forever?Heck yeah! Here’s where I start. I sleep! Tired or not, depressed or not, my deep sleep is the place I start. Self-care, boundaries, and rest. I don’t need to earn, they are the natural states I was ripped off of. I don’t call myself manic for my great ideas. I own my brilliance. But I pick them one by one and contain myself with discipline and ask for help when I want. I am beyond those checklists of symptoms and the labels been put on my every action. I speak up, stand up for myself and do the same for everyone. “I carefully listen to the joys and waves of laughter and the cries of those who had been silent for a while as I march on. Those ‘silenced’ will roar one day to their glory, and in their roar, the stigmatic words of hate, judgment, and despise will fade.” I know it’s a swing so come join me, why not! My lows are mine, my highs are too. Going so deep in my life would be impossible, if it weren’t for this Bipolar Disorder we call. What if I am just wired differently, like so many are. My anxiety is my yearning, my depression is my cry for rest, my mania is my higher-self. All this magic is real…as real it could be. And even if it is an illusion, it is a lucky one. P.s. stepping out of my comfort zone into the comedy zone.My biggest inspiration is Tim Ferriss who flipped his bipolar into learning everything he could do. One thing he said that stuck with me: if you want something new don't go after what's already created. Create something YOU need the most. For me, I stepped out of my comfort zone and onto the stage. I stood up and started making jokes about being bipolar. My mother couldn't stop laughing nor could the audience. But this was as much for me as it was for them, if not more so. I hope you enjoy.
12/8/2021 fighting through Hell as a child to emerge an empowered woman: the grit and resilience of a true mental health superhero, Meagan CopelinRead Now [TRIGGER WARNING: SH, SA, R*PE, ED] i have to fight through hell to become the EMPOWERED WOMAN i am today.
BEING BORN WITH GRIT, DETERMINATION AND FIGHT DOESN'T MATTER WHEN YOU'RE BORN TO TEENAGE DRUG ADDICTSAs a young girl, growing up in the city of New Orleans, I was always determined to be the very best and to never give up despite my obstacles. In fact, my aunts and uncles nicknamed me “Maybe Tomorrow” as they saw determination and grit from the moment I was born. My great-grandmother, Anna Copelin, who we called Mother Anna, holds a special place in my heart. Mother Anna passed away when I was 3 years of age, and although I do not remember much about her, I do know she still guides me and watches over me daily. She has truly been my guardian angel. My mom and dad were teenagers when I was born. I was primarily raised the first 3 years of my life by Mother Anna and my great grand-father, Daniel Copelin (Granddaddy Copelin), not because they wanted to but because they needed to. Even born as a premature baby, I had so much fight in me. I was a very small baby, with a big forehead (LOL). My great grandparents were full of love. The greatest memories I shared with Granddaddy Copelin was us sitting at the kitchen table eating stale ginger snaps and cold hot dog links. For some reason, my granddaddy loved giving us grandkids stale snacks. I still smile thinking about how my granddaddy enjoyed a snack that I found very unpleasant, but I still enjoyed spending time with my love. He was the first man that I ever loved, and he showed me love as I didn’t grow up with my dad in my life, so my granddaddy and certain uncles were there for me. My birth mom was in and out of my life and was extremely unstable. I remember when I was around 6 years old, she was involved in an unstable relationship with a man, and he got so mad at her that he hit her in the head with a car jack. She needed over 200 stitches. That was very scary to watch. I really think I started to experience mental health issues around that time or maybe earlier, starting around the age of 5. My dad disappeared when I was around 7 years old. I didn’t remember him and never cared to find him. I did start asking about him later but remembered that the other men in my life made sure I was good. (I am happy. I never had daddy issues thank goodness.) My mom and dad were both crack heads. I mean call it like you see it. They abused drugs heavily. I saw my mom take drugs, snort crack, and sell her body. I was young seeing all of this. WTF. No child should ever have to live through this hell.My mental health was spiraling out of control. I was starting to act out and cut myself. I was a child. Why was I seeing this shit? At the time, I never realized this was a sickness she possessed and for years I did not like her. I hated her. I didn’t want a relationship with her. I even told people she had died. I was angry so anything I said at that time I meant it. She was fucking up my mental health. I was depressed, had PTSD, was wetting the damn bed, experiencing an eating disorder, etc. I was a child. No child should ever have to experience this, no matter what. I WAS MAD at that time. My mom had lots of men in her life, and I mean LOTS of men. She would meet a man on Wednesday, and we would be living with him on Friday. I watched my mom experience lots of pain from men, from being abused to assaulted. She was on drugs and gone for days. There were times I didn’t see my mom for days, even weeks. This was traumatizing for myself as well as my brother and sister. My mental health was spiraling out of control. I was cutting myself and biting my nails down to the skin. I was going through hell. getting held down, raped and pimped out by your mother when eight seriously fucks with your mental healthAt the age of 8 years old, I was raped multiple times by my mom’s boyfriend. I think he was boyfriend number 500 of that year. I loved school and would go right to school after being raped by that ugly old ass monster. He smelled like grease and molded bread. He was a PIMP and would have sex with prostitutes before and after he raped me. My mom was aware of this but when drugs take over your life, that is typically the focus and not anything else around you. He told me not to tell anyone, and he even told me that he would tell her and that she wouldn’t do anything. The nerve. And he was right: I told her and nothing was done. These two were really messing with my PTSD. Severe depression was kicking in. Crack and cocaine are truly a hell of a drug. at age of 12, diagnosed with clinical depression, ptsd, anxiety, eating disorder, ocd, and behavioral and emotional disorder. thanks mom.School was my safe haven and even though I was bullied daily, I still went with dirty ass clothes and cuts on my body. I should have been playing with barbie dolls and eating dinner at the table with a normal family, but I was facing severe trauma at 8 and 9 years old. I eventually moved in with an abusive aunt, who would beat me with a broom and make me sleep in my own urine as I was still wetting the bed from severe trauma. I was suffering and going downhill. After two years or so, I had an opportunity to move with another aunt who changed my life. That aunt saw that I needed help and sent me to see a licensed psychiatrist. At the age of 12, I was diagnosed with clinical depression, PTSD, anxiety, an eating disorder, a behavioral and emotional disorder, and OCD. I was provided a prescription for mental health medication as well. learning to forgive, not for her, but for me.For years, I did not like my mom and didn’t see her again until I was 20 years old. I had to really learn forgiveness and it was hard. I sought counseling and joined a church to help me learn how to forgive my mom. I finally forgave her about 7 years ago. I am now 40. I realized that forgiving her was not about her but about me. And about freeing me. To move on and succeed in life, I had to learn the power of forgiveness. That was truly a process for me. I had to be open and understanding. I had to place myself in her shoes in order to understand her struggles. I didn’t have to have a relationship with her to forgive her. It felt good to rid that baggage that was holding me back for years. The act that hurt me will always be with me as I have that right, but forgiveness has lessened its grip on me. Forgiveness has allowed me to led with understanding in my personal life, as well as show empathy and compassion for my parents, as well as others around me. How can you improve your child's mental health? your child deserves it.One of the best things you can do to keep your child mentally healthy is to take care of your own mental health. As a parent, it is important that you protect your child and never allow them to be placed in situations that may harm them and scar them for life. A child needs to be a child and do things that children do, such as playing with dolls and car toys. Children are innocent.
Parents should also have a basic understanding and answers to questions such as what mental illnesses are, who can get them, what causes them if that is known, how diagnoses are made, and what treatments are available. Do your homework. Your child deserves it. i was put on this earth for a reason. speaking up about stigma is my gift. It is my calling.When I share my story with others, I always say that I am happy I have been through the things I have been through. My reason is because I believe GOD knew I could handle this. I am not my parents and never inherited any of their traits or habits. I was placed on this earth to help young girls and women all over the world share their story. Speaking up regarding the stigma of mental health is my gift. I was meant to do this. If you're thinking about hurting yourself, are worried about a friend or loved one, or would like emotional support, the Lifeline network is available 24/7 at 1-800-273-TALK (8255). AuthorDr. Meagan T. Copelin is the Supporting US Chair of Accelerating Mental Wellness, a social-justice campaign to co-create stigma free workplaces built on a foundation of empathy with needed mental health supports and programs. 12/5/2021 a call for social justice and STigma-Free Workplaces: WE get fired because of our mental illnesses BUT only we deal with STIGMA'S POISONous WRATH AND true depths of ENSUING SUFFERINGRead Now resilience built up in childhood. check. higher education underway. check. then, a series of weird events started happening.I had a very good childhood with loving parents and friends. I was bullied a little at school. But that gave me some resilience and taught me self dependence at a very early age. I was a straight A student and excelled at my studies. I got my Bachelors and then pursued a Masters in Computer Science from the best college in India. Being an INFJ, I was always a self-starter and figured out solutions to problems myself. Then, a series of weird events started to happen to me. In my last semester of graduate school, other students started noticing a change in my behavior. A calm, introverted kid was now fighting with everyone, verbally, not physically. I was much more irritable and got angry at the slightest of things. I was unaware at that time of exactly what was happening. i soldiered on, landing my first professional job. But, quickly burnout after being expected to work long hours, becoming nonfunctional for months.I started my internship at a game development company in 2014 where I was expected to work long hours. I was not performing at optimal levels and after 6 months, I experienced my first severe burnout. I came home severely depressed. My parents supported me. I was nonfunctional for months. My neighbors started noticing I was not getting out of the house. They did their best to try and talk to me. With that said, being in episodes spoiled my relationships with almost everyone. Yet, still I couldn't really figure out what exactly was happening to me until I had a lightbulb moment. My Lightbulb Moment. I realized I needed treatment to survive. And, I got THAT AND MORE: a bipolar 2 diagnosis and A LITHUM Prescription. check.I was lost in the darkness, struggling to figure out what was wrong with me. Grasping at straws, I went online and started reading and joined online forums. I read the DSM. I did research. I read blogs. That all led me to finally going to see a psychiatrist. After asking me questions during a one-hour consultation, he diagnosed me with Bipolar 2 and put me on Lithium. After three months of Lithium, I got a little stability and decided to give work another go. back to work ONLY TO HAVE my hard-fought stability snatched away. CEO discovers MY bipolar disorder. I'm fired.I got a job as a Junior System Admin two blocks from my house and worked there for almost 2 years. It was a mid-sized company with 150 employees. I had very good relationships with everyone and helped everyone with their computer issues. Then, the CEO finds out about my bipolar disorder and fires me two weeks later. Even to this day, I still get calls from the IT department asking for help with IT problems. I still offer give solutions. I Enter a stigma-free workplace at last. My stability, balance and SENSE OF worthiness RETURN.Then, I got a job at a chain of salons as an IT Manager. It had 3 branches for which I was managing the entire IT and digital marketing. This time, however, my boss was very supportive and helped me in every way to become productive. But due to COVID, he had to shut down two of the branches and laid off people. But he has always stayed in touch, even to this day. "To me stigma-free workplaces are built on foundations of people understanding the need for inclusivity and empathy. My third and current job was found via LinkedIn. I applied to a Denver-based company and the Founder interviewed me for an IT Manager position but gave me the Project Manager position. I got a few episodes during this job but my company supported me when they knew I had bipolar disorder. Medications Taken to date to see me through this journey. Did I have to go through all this? I had seen a severe form of illness but I could manage it and most people couldn't tell (or were not telling me) that I have such a severe condition. I had taken almost every medication over the years, which is generally prescribed for bipolar. I can't help but wonder if my journey would have not been as arduous if not been for stigma in the workplace; and if perhaps I would have found the perfect cocktail for treating my bipolar sooner. You see it is not easy or particularly fun to have to try all these different medications as you cycle up and down and as society pushes us up and down with stigma.
My most irritable symptoms were hand tremors and throbbing headaches. I still have these. How do I COPE? BY FIGHTING BACK. AND BY GIVING BACK TO OUR COMMUNITY.Cancer doesn't just go away, nor does bipolar disorder. You have to find methods in order to survive. I learnt coping mechanisms for my illness at a very early stage. I could tell when my moods were swinging and took immediate action. Other coping mechanisms included:
But, the best coping mechanism for me has been and still is helping people. That naturally lifts your depression. I have been helping people for many many years with their IT stuff and with my mental health advocacy work. LIKE AIR POLLUTION, STIGMA IN OUR WORKPLACES IS POISONING US CAUSING BOTH PHYSICAL AND EMOTIONAL SUFFERING. LIKE A CLASS ACTION LAWSUIT, WE ARE FILING A SOCIAL ACTION LAWSUIT. WE ARE TIRED OF BEING FIRED.Most recently, I have become the Chair in India for Accelerating Social Good's social-justice campaign, Accelerating Mental Wellness, to co-create stigma free workplaces built on a foundation of empathy with needed mental health programs and supports in place. Why? Because it is unjust for people like me to get fired simply because I have bipolar disorder. I see this as analogous to a class action lawsuit in America. Like a social action lawsuit in a way. People are poisoned by stigma. In a class action lawsuit, I understand people are literally poisoned by pollution so they come together and file a lawsuit to get reimbursed for medical bills and for their suffering, the punitive damages.  But we are not filing a class action lawsuit. We are not taking this to court. We are taking it to the people. We are taking it to to you. We are asking you to lean in and listen to the human case, our stories. How is this any different for those of us with bipolar or other mental illnesses (read serious brain disorders) who are being fired? Is stigma in the workplace not poisoning us to? Are we not also feeling physical pain? Trust me, having to go on med and after med to try to regain your footing after being fired does cause much physical as well as emotional pain. We too are suffering. Where is our justice? Who is standing up for what is right? Who is advocating for change? I am. Accelerating Social Good is: Founder and CEO and Founder, Kerry Martin, supported by Meagan Copelin, chairing in the United States, COO Erin Macauley chairing in Australia, and Natasha Tracy chairing in Canada. They are leading mental health advocates and they all have lived experience too. They also have their own stigma stories, some harder to read than mine. But it's not just us. There are many others who agree stigma in our workplaces is discriminatory, unjust. And, not just for those with a serious brain disorder such as bipolar but unjust for every single human regardless of your physical or mental health condition, visible or invisible, and regardless of the color of your skin or your sexual preference. It's unjust period. Please visit our Wall of Solidarity, made up of everyday people like you and me. People who have stepped up to join us in our campaign. We call them our stigma-fighter superheroes as by uploading their selfies to our wall they are helping us take another brick out of the wall of stigma and sending a clear message that we want the wall taken down. Finally. These are not just concerned citizens, but global diversity, inclusion and equity leaders, best-selling authors, mental health advocates, podcasters, nonprofit leaders, and those that suffer from mental health conditions. I hope that others will join us in our grassroots campaign to eradicate stigma in our workplaces and put an end to the discrimination. And, to finally provide urgently needed mental health programs and supports in our workplaces for all who are suffering. We are all humans worthy of support, not worthy of being poisoned by stigma. No one should get fired because they have a mental illness. This discriminatory practice must be stopped. AuthorSHitesh Gupta, India Chair, Accelerating Mental Wellness, A Global Workplace Cause-Advocacy Initiative Sponsored by Accelerating Social Good with contributions by Kerry Martin, Chief Purpose Officer and US Chair. 11/24/2021 WE aRE here to build a world where all children flourish but first we need STIGMA-FREE workplaces: FOUR simple ways you can helpRead Now why i am doing this accelerating mental wellness campaign FOR WORKPLACES. what is your why?Please allow me to introduce my why, the inspiration that drives me to work so hard on this campaign: Sara. We have hashtags for one another, #saraslight and #kerryshope. Accelerating Social Good collaborates with causes to build a world where the mental healthcare system doesn't let anyone down. A world where all our children can flourish. To enable all lights to shine, we simply must have work settings that support and empower people, environments wherein my precious Sara's light is allowed to illuminate as bright as possible. It is for Sara, who is now 24, and her beautiful friends, that I dedicate much of my time to ensure this cause-advocacy campaign exceeds our expectations. What about you? Is creating stigma-free workplaces built on a foundation of empathy, caring, compassion important to you too? Should workplaces be providing mental health programs and supports? What is your why? Please consider joining us. Stand with others and share your selfie, and/or share your story. We are simply stronger as advocates and concerned citizens when we stand together. If we are here to affect social change, this is how we can do it. Together. help write stigma-free story with an empathy plot. a story of hope. let's co-create workplaces we all can flourish.If mental health advocates collaborate, we can interweave a more inclusive story both persuasive enough to change society and powerful enough to shine a light on what the future should look like. A future of no stigma. A future with where we lose fewer precious souls far too soon. A future of mental wellness. A future of hope. A future where we all can flourish. Let's work together to create stigma-free workplaces, rebuilt on a foundation of empathy and caring, by sharing our lived experiences. A key to ending mental health stigma (read systemic discrimination) is to humanize it with storytelling.
BUT WE CAN'T DO THIS ALONE. WE NEED YOUR HELP.This is a rallying cry to advocates and concerned citizens to come together. To share our selfies and our stories in a collaborative and coordinated campaign to accelerate social change on behalf of those who are suffering in silence and shame. With must step up and speak out, a calling more salient in light of the Great Resignation. Whilst it is easy to build a business case for workplaces to integrate mental health access and programming as a benefit (and we intend to do so), let's also come together to do the hard work. Let's build a human case for rebuilding our workplaces on a foundation of empathy and caring. If you are a mental health advocate, please consider joining us and raising your voice. Let's all stand up and be heard. And together, be so loud that eventually they must not only listen but TAKE A PLEDGE to either acknowledge the importance of this initiative or take concrete steps to create a stigma-free workplace with appropriate mental health programming and supports for employees. More on this to come in 2022. FOUR ways you can help
AuthorKerry Martin, Sara's Number 1 Fan, CEO & Founder, Accelerating Social Good; US Lead Chair, Accelerating Mental Wellness Social Change Campaign. |
Archives
February 2023
Categories
All
|





 RSS Feed
RSS Feed